
 |
|
Juliana Romanato1; Marcos Roberto Menezes2,a; Allan de Oliveira Santos3,4,b; Regis Otaviano Franca Bezerra5,c; Mariana Cunha Lopes Lima6,7,d; Elba Etchebehere8,9,e
ABSTRACT
OBJECTIVE: To determine whether 18F-fluorodeoxyglucose positron emission tomography/computed tomography performed immediately after percutaneous ablation (iPA18F-FDG PET/CT) is useful in evaluating the outcomes of the procedure. MATERIALS AND METHODS: This was a retrospective study of 20 patients (13 males, 7 females; mean age, 65.8 ± 12.1 years) submitted to percutaneous ablation of metastases. All of the lesions treated had shown focal uptake on a 18F-FDG PET/CT scan obtained at baseline. The primary tumors were mainly colorectal cancer (in 45%) or lung cancer (in 40%). iPA18F-FDG PET/CT was performed to identify any residual viable tumor cells. The treatment was considered a success (no viable tumor cells present) if no uptake of 18F-FDG was noted on the iPA18F-FDG PET/CT scan. RESULTS: Twenty-six lesions were submitted to percutaneous ablation with either cryoablation (n = 7) or radiofrequency ablation (n = 19). The mean lesion diameter was 2.52 ± 1.49 cm. For the detection of viable tumor cells, iPA18F-FDG PET/CT had a sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of 66.7%, 95%, 88.5%, 80%, and 90.5%, respectively. There was a significant correlation between the iPA18F-FDG PET/CT findings and the results of the follow-up studies (kappa = 0.66; p < 0.01). CONCLUSION: iPA18F-FDG PET/CT studies appear to constitute a useful means of evaluating the outcomes of percutaneous ablation. By detecting residual viable tumor cells, this strategy might allow early re-intervention, thus reducing morbidity. Studies involving larger numbers of patients are needed in order to confirm our findings.
Keywords: Fluorodeoxyglucose F18; Positron-emission tomography/methods; Tomography, X-ray computed/methods; Ablation techniques; Cryosurgery/methods; Radiofrequency ablation.
RESUMO
OBJETIVO: Demonstrar se a tomografia por emissão de pósitrons acoplada a tomografia computadorizada usando-se fluorodesoxiglicose marcada com flúor-18 realizada imediatamente após ablação percutânea (iAP18F-FDG PET/CT) pode ser útil na avaliação do resultado desse tratamento. MATERIAIS E MÉTODOS: Foram avaliados, retrospectivamente, 20 pacientes (13 homens e 7 mulheres; média de idade: 65,8 ± 12,1 anos) submetidos a ablação percutânea de metástases apresentando captação de 18F-FDG no exame de PET/CT. Os tumores primários foram, principalmente, câncer colorretal (45%) ou câncer de pulmão (40%). A iAP18F-FDG PET/CT foi realizada para avaliar tumor residual viável. O tratamento foi considerado sucesso (sem lesão viável) se nenhuma captação de 18F-FDG fosse observada na iAP18F-FDG PET/CT. RESULTADOS: Vinte e seis lesões foram submetidas a ablação percutânea por meio de crioablação (n = 7) ou radiofrequência (n = 19). O tamanho médio das lesões era de 2,52 ± 1,49 cm. A iAP18F-FDG PET/CT detectou tumor viável com sensibilidade, especificidade, acurácia, valor preditivo positivo e valor preditivo negativo de 66,7%, 95%, 88,5%, 80% e 90,5%, respectivamente. Houve correlação significativa entre os achados da iAP18F-FDG PET/CT e os resultados do seguimento clínico dos pacientes (kappa = 0,66; p < 0,01). CONCLUSÃO: A iAP18F-FDG PET/CT é capaz de avaliar o resultado da ablação percutânea e poderá permitir reintervenção precoce de lesões residuais viáveis, reduzindo a morbidade. Um número maior de pacientes é necessário para confirmar esses achados.
Palavras-chave: Fluordesoxiglicose F18; Tomografia por emissão de pósitrons/métodos; Tomografia computadorizada/métodos; Técnicas de ablação; Criocirurgia/métodos; Radiofrequência.
INTRODUCTION For cancer patients, the primary treatment with curative intent is surgery. However, some patients-such as those whose clinical condition make them poor candidates for surgery and those whose lesions are located at difficult-to-access sites-are treated with percutaneous ablation. This approach is becoming more common in clinical practice because of its minimally invasive nature and low complication rates. For situations such as those cited above, a wide variety of percutaneous ablation techniques have been developed(1). For primary tumors and metastases of solid tumors, the use of cryoablation or radiofrequency ablation has increased the possibility of cancer control in patients who are not good surgical candidates. Percutaneous cryoablation is a minimally invasive technique that consists in image-guided insertion of probes into the tumor and the subsequent application of successive freeze-thaw cycles, reaching temperatures as low as -140ºC. This strategy causes tissue destruction by breaking cell membranes through phase change and intracellular ice crystal formation. The freezing mechanism is due to the thermodynamic property of argon, which undergoes severe heat loss during its expansion in a closed chamber (the Joule-Thomson effect). Thawing is achieved by replacing the argon with helium, whose expansion has the opposite effect, heating the system. At the beginning of the freeze cycle, an ice ball forms at the end of the probe. The growth of the ice ball can be controlled by adjusting the probe parameters and can be accurately monitored with computed tomography (CT). The outermost layer of the ice ball, as visualized on CT or magnetic resonance imaging (MRI), is less effective than is its central portion and must therefore be at least 0.5 cm beyond the limits of the target tumor. The ability to view and monitor the expansion of the ice ball by CT or MRI allows the treatment of the entire tumor to be optimized and reduces the risk of injury to adjacent structures. The cryogenic damage occurs not only at the cellular level; it also affects the microcirculation surrounding the target tissue. In the days that follow cryoablation, the damage caused by the freezing of the tissue promotes platelet aggregation and ischemic injury, leading to tissue necrosis(2). Cryoablation has been used successfully to treat a variety of benign and malignant diseases in different locations, including the liver, kidneys, breast, and prostate(3-6). Radiofrequency ablation is performed by introducing energy into the tissue through an active electrode, causing the ions within the tissue to vibrate under alternating currents. That movement of particles results in heating of the tissue by friction reaching temperatures above 60ºC, causing coagulation necrosis around the electrode. The advantage of this thermal intervention is its capacity to heat the tissue to a lethal temperature at a specific anatomic location(7). After percutaneous ablation, it is crucial to evaluate the treatment outcome, in order to avoid recurrence. Follow-up studies with CT and MRI are not able to differentiate between scar tissue and viable tumor cells, particularly in the lungs, and early follow-up studies typically produce inconclusive findings, regardless of whether the technique employed was cryoablation or radiofrequency ablation(8,9). Whole-body studies with 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) have been used in a variety of malignancies(10-12). The technique has been used successfully to monitor treatment response after chemotherapy and radiosurgery, either visually or by calculating standardized uptake value (SUV) to quantify the response(13). Because coagulation necrosis does not take up 18F-FDG(14), the use of 18F-FDG PET/CT may be an efficient means of evaluating the outcome of percutaneous ablation. Viable tumor cells can be detected by 18F-FDG PET/CT earlier than morphological changes can be depicted by CT and MRI. However, 18F-FDG is not a specific tracer for viable tumor cells and can be taken up by inflammatory processes. Consequently, there can be 18F-FDG uptake in the tissue surrounding the treated region, due to the inflammation induced by percutaneous ablation. However, such inflammation does not develop immediately after percutaneous ablation, appearing only hours later. Therefore, the optimal time to perform 18F-FDG PET/CT imaging of patients who have undergone percutaneous ablation is within the first few hours after the procedure(15). The purpose of this pilot study was to determine whether 18F-FDG PET/CT performed immediately after percutaneous ablation (iPA18F-FDG PET/CT) is an efficient means of evaluating the outcome of percutaneous ablation. To that end, we reviewed the records of a sample of patients in whom this strategy was employed. MATERIALS AND METHODS Patient data This was a retrospective study of patients who were submitted to percutaneous ablation. The local institutional review board approved this study (IRB Reference No. 2013-19). We included all patients with solid tumor metastases from various types of primary tumors in whom percutaneous ablation was indicated and there was focal uptake of 18F-FDG prior to percutaneous ablation. The inclusion criteria were having undergone percutaneous ablation (cryoablation or radiofrequency ablation), having had a baseline 18F-FDG PET/CT scan within the last 30 days prior to percutaneous ablation, and the baseline scan having shown 18F-FDG uptake in the solid metastasis targeted. Patients in whom there was a change in the chemotherapy regimen were excluded, as were those in whom chemotherapy was initiated during the first 6 months after percutaneous ablation because of recurrence at sites other than the site targeted in the percutaneous ablation. Each patient underwent another iPA18F-FDG PET/CT, the intent being to evaluate the outcome of the procedure. The treatment was considered a success (no viable lesion remaining) if no 18F-FDG uptake was seen on the iPA18F-FDG PET/CT images. Regardless of the iPA18F-FDG PET/CT results, patients were not submitted to a new intervention and were followed through clinical examination and imaging modalities. The follow-up studies were performed with 18F-FDG PET/CT, MRI, or contrast-enhanced CT. If suspicious uptake was noted on the iPA18F-FDG PET/CT scan, the patient in question was submitted to closer surveillance. Re-intervention occurred only if one of the follow-up studies revealed abnormalities. Baseline 18F-FDG PET/CT studies The baseline 18F-FDG PET/CT studies performed at our institution were acquired with the protocol described below. All of the baseline scans were performed within the last 30 days prior to percutaneous ablation. Patients were required to fast for 6 h prior to the injection of 18F-FDG, in order to achieve a blood glucose level below 140 mg/dL. All patients received 18F-FDG at a dose of 7.77 MBq/kg (0.21 mCi/kg) while resting in a dark, quiet room. Whole-body PET/CT scans were acquired 60 min after 18F-FDG injection. The images were acquired on a high-resolution imaging platform (Biograph TruePoint; Siemens Medical Solutions, Knoxville, TN, USA) with lutetium oxyorthosilicate crystal detectors, 16-slice CT detectors, and a spatial resolution of 4.2 mm. The image post-processing was performed with Syngo MultiModality Workplace software (Siemens Medical Solutions). The PET images were acquired after the CT images (5 min per bed position). Images were submitted to iterative reconstruction in the axial, coronal, and sagittal planes, CT being used for attenuation correction. The maximum SUV (SUVmax), was calculated for each lesion. Two experienced nuclear medicine physicians and a radiologist analyzed the images. Discordant findings were reviewed by a third experienced nuclear medicine physician. iPA18F-FDG PET/CT studies To perform the iPA18F-FDG PET/CT studies, the patients were referred to the Division of Nuclear Medicine 1-14 h after the percutaneous ablation procedure. The time to perform the iPA18F-FDG PET/CT study after percutaneous ablation varied, depending on the condition of the patient after the percutaneous ablation procedure. Patients were required to remain in a fasting state for 6 h after percutaneous ablation (i.e., 6 h prior to the injection of 18F-FDG), in order to achieve a blood glucose level below 140 mg/dL. All patients received 18F-FDG at a dose of 7.77 MBq/kg (0.21 mCi/kg) while resting in a dark, quiet room. Images of the lesion submitted to percutaneous ablation were acquired 60 min after 18F-FDG injection. The images were acquired and reconstructed on the same PET/CT equipment described above. The SUVmax was calculated for each lesion. The two nuclear medicine physicians and radiologist who had evaluated the baseline 18F-FDG PET/CT scans also analyzed the iPA18F-FDG PET/CT images, and discordant findings were reviewed by a third experienced nuclear medicine physician. The SUV of the baseline 18F-FDG PET/CT was not used for comparison with that of the iPA18F-FDG PET/CT, because some of the baseline studies were performed on PET/CT equipment at different institutions. Percutaneous ablation procedures Prior to each percutaneous ablation procedure (radiofrequency ablation or cryoablation), the patient underwent a blood coagulation assessment, consisting of a complete blood count, as well as the determination of hemoglobin, hematocrit, prothrombin time, partial prothrombin time, and platelet count. All percutaneous ablations were performed under general anesthesia with endotracheal intubation. In the operating room, the ablation probes were carefully placed within the tumor under ultrasound, CT, or MRI guidance. Prior to needle insertion, the point of entry, the safest trajectory, and the final position of the needle were carefully planned. Once the needle had been inserted, the point of entry was confirmed by axial images of a contrast-soaked cotton pledget that was placed over the lesion. If needed, local anesthesia was given along the needle tract up to the surface of the target organ. In cases of multiple lesions in the liver, the lesions were submitted to percutaneous ablation only if they were at least 5.0 cm apart. Lesions in the lungs were submitted to percutaneous ablation if they were located more than 1.0 cm from the hilum. Whenever aerated lung tissue was traversed, a thoracic surgeon would insert an intercostal drainage tube for the management of large pneumothoraces. Radiofrequency ablation procedure In the patients who underwent radiofrequency ablation, we used an electrosurgical radiofrequency generator (1500X; RITA Medical Systems, Fremont, CA, USA). The generator employed provides monopolar radiofrequency and delivers 150 W of power in most modes with up to 200 W of power in the infusion mode. The radiofrequency electrodes consist of a deployable array of hooks, all equipped with thermocouples. Those are connected to a main cable and deliver radiofrequency energy from the generator to the electrode. The dispersive electrodes complete the electrical circuit and provide the return path for the radiofrequency energy applied by the device. The type of needle electrode used was determined by the size, location, and geometry of the tumor. Subsequently, the radiofrequency electrode was positioned along the anesthetized tract such that its tip was approximately 1.0 cm from the geometric center of the lesion. The expandable array of electrodes was deployed in stages, and the tumor was progressively ablated. Tumor ablation was performed by applying sustained progressive heating. The entire tumor, together with a 1.0 cm margin of normal tissue, was ablated. The radiofrequency ablation session typically lasted 10-15 min. Treated areas had 0.5-1.0 cm tumor-free margins. Cryoablation procedure The cryoablation system (Cryocare; Endocare, Irvine, CA, USA) included a probe with a 2.4-mm outer diameter. The number and size of the probes used were based on the size and location of the tumor, as well as on the anticipated geometry of the ice ball. In general, more than one probe was used when treating larger tumors (because of the larger ice ball formation) and when treating lung lesions near vessels (to better overcome the heat-sink effect). Tumor ablation was typically performed with overlapped sessions or with an ice ball margin. The intention was to ablate the entire tumor with a tumor-free margin of 1.0 cm. Statistical analysis We calculated the proportion of cases in which the percutaneous ablation was successful, in order to determine the agreement between the iPA18F-FDG PET/CT result and that of the follow-up study (performed approximately 6 months later). The kappa coefficient was calculated. The mean size of the lesions submitted to cryoablation was compared with that of the lesions submitted to radiofrequency ablation using the Student''s t-test. RESULTS Percutaneous ablation was performed in 20 patients (13 of whom were male), ranging in age from 43 to 83 years (mean age, 65.8 ± 12.1 years). A total of 26 lesions were submitted to percutaneous ablation: cryoablation (n = 7) or radiofrequency ablation (n = 19). The mean lesion diameter was 2.52 ± 1.49 cm. Primary tumors were mainly colorectal cancer (in 45%) or lung cancer (in 40%). Other malignancies included sarcomas, thymomas, malignant melanomas, and ovarian cancers. Metastatic lesions were located in the liver (in 50%), the lungs (in 30%), and other sites in the abdomen (in 19.2%), including intraperitoneal and retroperitoneal lymph nodes (Table 1).
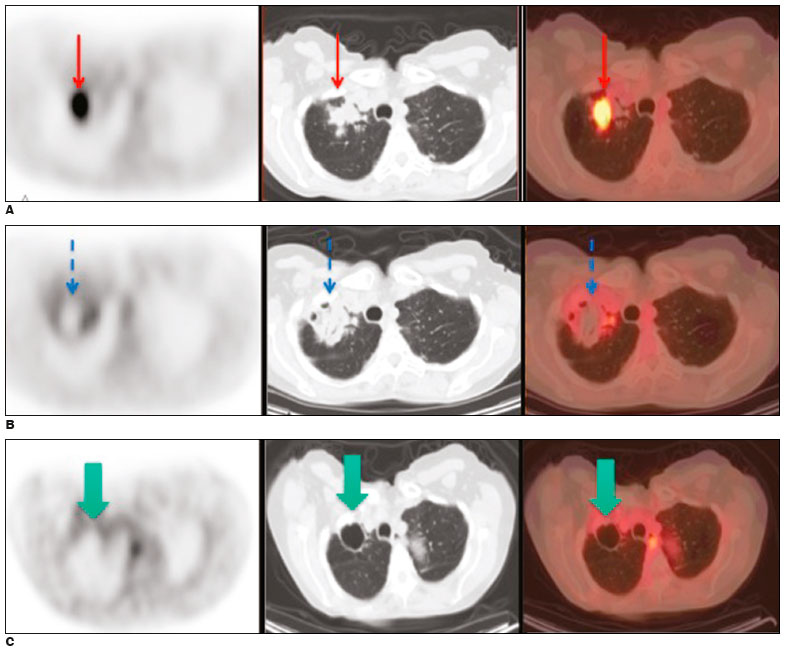 Figure 1. A: Baseline 18F-FDG PET/CT images of a lung metastasis, performed prior to cryoablation, showing marked focal uptake within the lung lesion (arrows). B: iPA18F-FDG PET/CT scan acquired at 3 h after cryoablation, showing no 18F-FDG uptake within the lesion and a rim of uptake consistent with postoperative inflammation (arrows). C: Follow-up 18F-FDG PET/CT images and clinical examination performed at 6 months after the procedure, showing no signs of viable tumor cells (arrows).
Figure 1. A: Baseline 18F-FDG PET/CT images of a lung metastasis, performed prior to cryoablation, showing marked focal uptake within the lung lesion (arrows). B: iPA18F-FDG PET/CT scan acquired at 3 h after cryoablation, showing no 18F-FDG uptake within the lesion and a rim of uptake consistent with postoperative inflammation (arrows). C: Follow-up 18F-FDG PET/CT images and clinical examination performed at 6 months after the procedure, showing no signs of viable tumor cells (arrows).
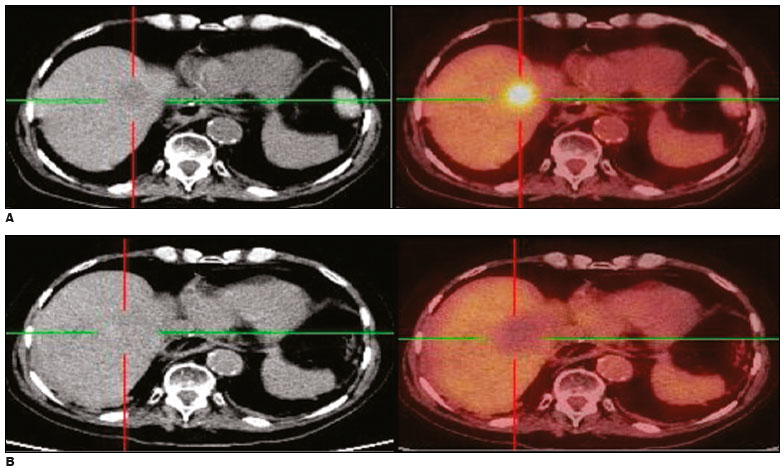 Figure 2. A: Baseline 18F-FDG PET/CT images of a liver metastasis demonstrating focal uptake. B: iPA18F-FDG PET/CT images, acquired at 5 h after radiofrequency ablation, showing no 18F-FDG uptake. Follow-up 18F-FDG PET/CT study, conducted at 6 months after the procedure, showing no signs of viable tumor cells.
Figure 2. A: Baseline 18F-FDG PET/CT images of a liver metastasis demonstrating focal uptake. B: iPA18F-FDG PET/CT images, acquired at 5 h after radiofrequency ablation, showing no 18F-FDG uptake. Follow-up 18F-FDG PET/CT study, conducted at 6 months after the procedure, showing no signs of viable tumor cells.
 Figure 3. A: Baseline 18F-FDG PET/CT image of a liver metastasis showing focal uptake (arrow). B: iPA18F-FDG PET/CT image, acquired at 4 h after radiofrequency ablation, showing a large region with no 18F-FDG uptake (curved arrow) and a small focal region with minimal residual uptake (dashed arrow). C: 18F-FDG PET/CT image, acquired 3 months after radiofrequency ablation, showing that the small focal region with minimal residual uptake had increased in size and metabolism, consistent with the presence of residual tumor cells (arrow). D: The patient was submitted to another radiofrequency ablation session. E: Image acquired at 14 months after the first procedure showing no signs of viable tumor cells.
Figure 3. A: Baseline 18F-FDG PET/CT image of a liver metastasis showing focal uptake (arrow). B: iPA18F-FDG PET/CT image, acquired at 4 h after radiofrequency ablation, showing a large region with no 18F-FDG uptake (curved arrow) and a small focal region with minimal residual uptake (dashed arrow). C: 18F-FDG PET/CT image, acquired 3 months after radiofrequency ablation, showing that the small focal region with minimal residual uptake had increased in size and metabolism, consistent with the presence of residual tumor cells (arrow). D: The patient was submitted to another radiofrequency ablation session. E: Image acquired at 14 months after the first procedure showing no signs of viable tumor cells.
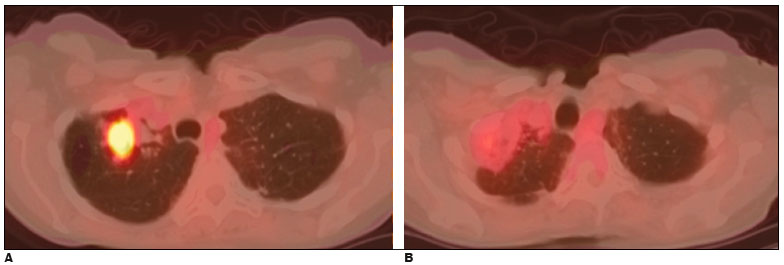 Figure 4. A: Baseline 18F-FDG PET/CT image of a lung metastasis from colorectal cancer. Cryoablation was performed. B: iPA18F-FDG PET/CT scan, acquired at 14 h after cryoablation, showing a rim of diffuse 18F-FDG uptake around the lesion with no clear uptake within the lesion itself. Despite the knowledge of the possible effect of inflammation of the surrounding tissue, it was not possible to conclude whether or not there were viable tumor cells present.
Figure 4. A: Baseline 18F-FDG PET/CT image of a lung metastasis from colorectal cancer. Cryoablation was performed. B: iPA18F-FDG PET/CT scan, acquired at 14 h after cryoablation, showing a rim of diffuse 18F-FDG uptake around the lesion with no clear uptake within the lesion itself. Despite the knowledge of the possible effect of inflammation of the surrounding tissue, it was not possible to conclude whether or not there were viable tumor cells present.
![]()
![]()
![]()

 PDF English
PDF English
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket